First of all, apologies for not blogging in a while. Between practicing law during the day and two EMS roles that keep me busy, I tend to forget that I have a blog and only will wander over here when one of two things happen. One – when I get the email reminding me that I’ll be getting a bill for keeping the domain registration. Two – when something really inspires me. And right now, y’all are going to get both. And probably from both barrels.
This morning, I saw another one of those Twitter screenshots that goes viral around the EMS/emergency medicine/medical social media pages.
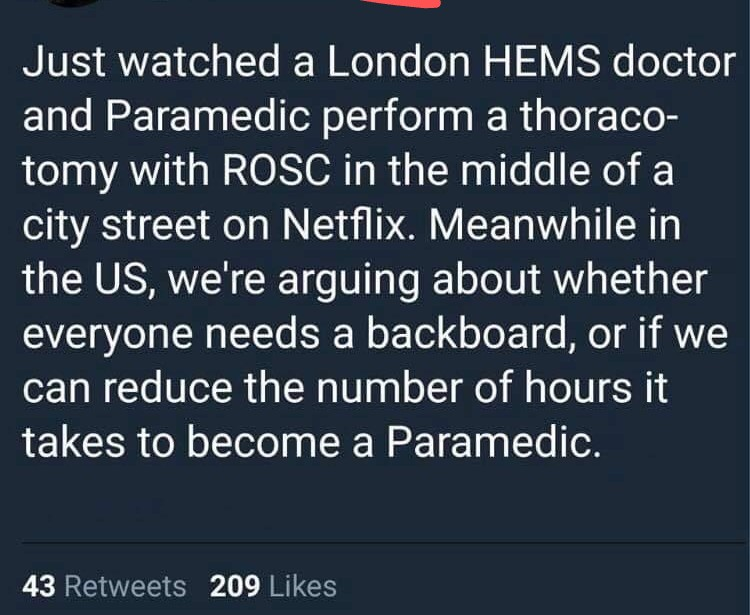
And said post upset and infuriated me. Not because of the truth or untruth of it, Rather, it’s trite and lacks understanding. So, as someone with quite a bit of education both in and outside of EMS and some experience with education and EMS policy, allow me to share my take.
Bluntly, I’m beyond tired of people comparing American EMS to EMS in any other country, particularly the United Kingdom, Australia, or Canada. All of these countries are dramatically different from the United States. Heck, compare EMS between different US states and you’ll see dramatic differences (Los Angeles County, California versus Texas – the land of delegated EMS practice.) Each of these countries have different forms of a national healthcare system and very different educational systems. (For example, an Australian bachelor’s degree is a three year degree as opposed to the typical four years here in the States.)
Bluntly, if American EMS is so awful, why does a large Louisiana-based private EMS concern keep getting Australian medics coming here? Could it be because maybe the grass isn’t necessarily greener in the Southern Hemisphere? The reality is that there’s a glut of degreed Australian medics and the jobs aren’t there.
If American EMS is so awful, where’s the peer reviewed studies comparing outcomes between American EMS and some of the countries with degreed medics? Most of the Med Twitter types that I see sharing these posts always want to “trust the science” and see the data. As of yet, I’ve not seen such data produced.
Oddly enough, American medics (well, excluding a few states that I won’t name like California) have a scope of practice that typically exceeds medics in these other countries. Securing an airway with paralytics, administering whole blood, and ventilators are common in progressive American EMS systems. In these other countries, they’re often reserved for graduate-level degree holding medics — or doctors. (Please note that, especially in the UK, flight crews are typically a medic and physician as opposed to our usual American model of a medic and a nurse.)
My blunt, candid take? A lot of these posts come from people who automatically assume that anything done outside of the borders of the United States is automatically better. Equally likely, these folks don’t understand the differences in EMS models, healthcare funding, and education that exist between the United States and these other countries. I’d also submit to you that many of these people haven’t had a great deal of exposure to EMS outside their own little corner of America — and assume that EMS is the same everywhere. It’s not
Can American EMS improve? Absolutely. Paramedicine shouldn’t be a jobs program for the fire union. Nor should it be delivered by the low bidder. And EMS providers of all levels shouldn’t be sitting in an ambulance for twelve hours a day driving all over town without an actual station to return to. Our education should not end at dropping the patient off in the emergency department. And we can fix much of this by beginning to educate the public about who we are and what we do.
That public outreach and education absolutely should NOT include selling American EMS short — and making us sound like the ignorant provincials that the Med Twitter illuminati think we are.