For those of y’all who know me away from this screen (and even for some of y’all who only know me online), you probably know that while my undergraduate degree is from the University of Texas, it’s not where I started my college career. I was honored to be appointed to the United States Naval Academy. (Just to humble brag a bit, I also had a senatorial nomination to the United States Military Academy.) I realized relatively soon that this was not the long term path for me. I have no regrets for following this path as I’d have always wondered what would have happened had I taken the appointment to a service academy.
What I did learn is that hazing is a real thing. The service academies have a long tradition of hazing for a variety of reasons. I think the key reason is tradition. Namely, “If I had to put up with this, so do the ‘new kids.'”
I won’t deny that there’s a place for creating high stress environments, holding people accountable, or using physical exercise as a form of “correction.” Truth be told, there’s more than a few times that I’ve wanted to use “knife hands” or a drill instructor style shark attack to drive a point home to someone who seems willfully clueless. In my attorney job, my colleagues in human resources tell me that’s not professional. In a fire or EMS environment, sometimes a pointed conversation is needed to drive home a point. And virtually no one will argue that there’s a need for strict discipline in a military environment, especially for initial training. I’m NOT going to be the one to argue that the SEAL’s infamous “Hell Week” should be replaced with “A Forty Hour Work Week That’s Less Than Pleasant.” Some environments demand this level of intensity.
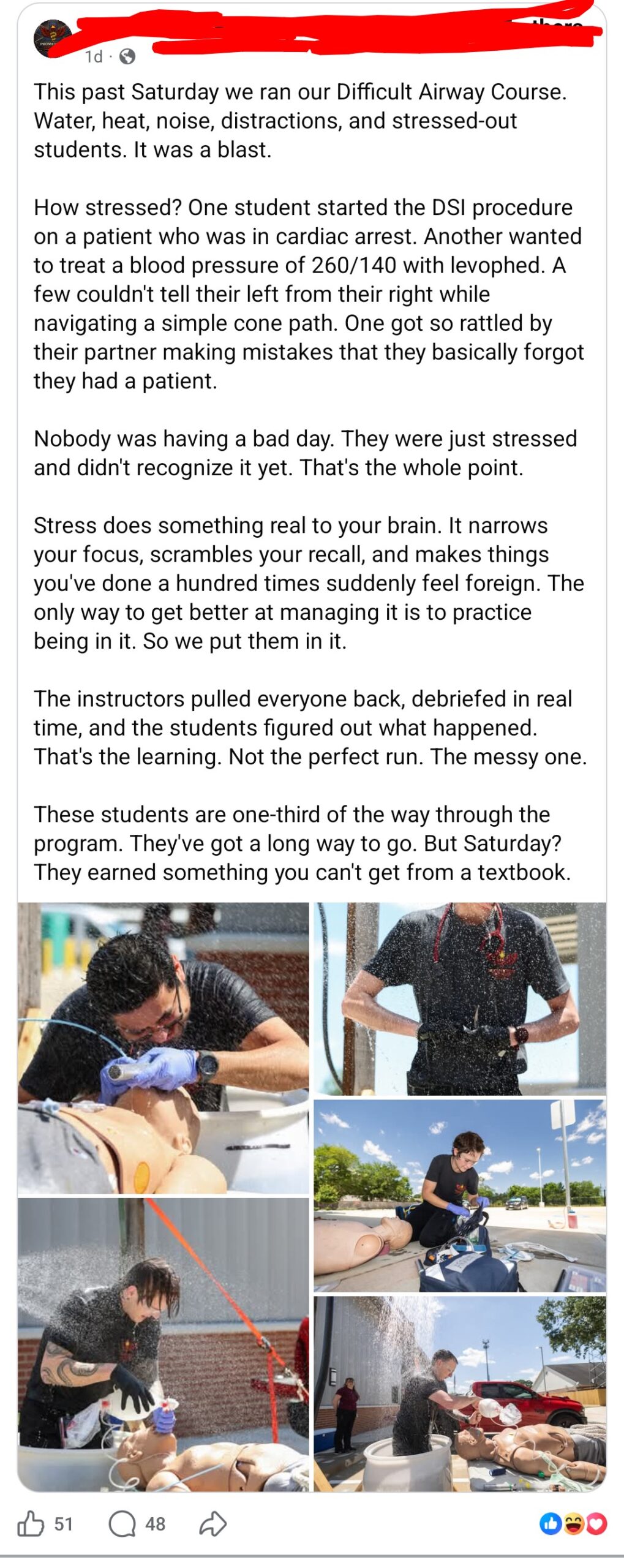
But I’ll tell you one place where this level of intensity is NOT needed. Emergency Medical Services. It’s not needed in initial EMS education. It’s not needed in a paramilitary style “academy” for new hires. Period. Yet, there are a few education programs that “brag” on it. Likewise with a few services who do a new hire academy for already certified EMTs and paramedics.
Right now, there’s an initial entry paramedic education program that’s advertising such hazing on their social media as part of a process to get their students to react to stress. They call it education. Pic below for proof.
The program is clearly proud of their educational efforts. While I am a lawyer, I’m not your lawyer. And I’m certainly not this program’s lawyer. What I can do is show you what Texas law defines as hazing, but this is only applicable in very specific academic or extracurricular settings. See Texas Education Code 37.151:
(6) “Hazing” means any intentional, knowing, or reckless act, occurring on or off the campus of an educational institution, by one person alone or acting with others, directed against a student for the purpose of pledging, being initiated into, affiliating with, holding office in, or maintaining membership in an organization if the act:
(A) is any type of physical brutality, such as whipping, beating, striking, branding, electronic shocking, placing of a harmful substance on the body, or similar activity;
(B) involves sleep deprivation, exposure to the elements, confinement in a small space, calisthenics, or other similar activity that subjects the student to an unreasonable risk of harm or that adversely affects the mental or physical health or safety of the student;
(C) involves consumption of a food, liquid, alcoholic beverage, liquor, drug, or other substance, other than as described by Paragraph (E), that subjects the student to an unreasonable risk of harm or that adversely affects the mental or physical health or safety of the student;
(D) is any activity that induces, causes, or requires the student to perform a duty or task that involves a violation of the Penal Code; or
(E) involves coercing, as defined by Section 1.07, Penal Code, the student to consume:
(i) a drug; or
(ii) an alcoholic beverage or liquor in an amount that would lead a reasonable person to believe that the student is intoxicated, as defined by Section 49.01, Penal Code.
I think twelve people who couldn’t get out of jury duty might well consider this to fit the definition of “hazing.” It’s rather fortunate for those conducting this program that the program does not fit the definition of an education institution. Having seen a few of the names involved, I’m surprised by some and sadly, not surprised by some of the other names.
And here’s a note. The other healthcare professions don’t do this. Sure, resident physicians work long hours. They work on call. But this is part of being a physician and it’s exposing them to this in an environment that is supposed to have guardrails. The only guardrails in this screenshot seem to be the sadists running this “education program.”
But it’s not just Texas. Another state believes this is acceptable in an educational setting. Granted, the paramedic education program is conducted by the EMS agency — in conjunction with that county’s police force.

A local-to-me EMS agency runs every group of newly hired EMTs and paramedics, regardless of their experience, through a new hire academy where they’re called “cadets,” subject to paramilitary style discipline and mandatory physical training. Call me crazy, but I’d rather these EMTs and paramedics learn the intricacies of their particular EMS system, receive a refresher on current medicine, and maybe even get a modicum of exposure to basic customer service skills.
Another EMS system that I’m familiar with had a field training officer who made his trainees do calisthenics prior to performing skills.
I ask one simple question. Who taught any of these people that this is acceptable in a training environment, let alone something you should be advertising? Because these people aren’t coming up with these things in a vacuum. Someone has taught them this is “ok.” Someone has normalized this. Someone has held this model up as the “way things ought to be.”
This is not okay. We cannot normalize abusing students and/or future colleagues. Period. Full stop. No exceptions. No explanations. Behavior like this needs to be called out. It needs to be shamed. And these people need to be promptly kicked out of our profession.
Want to fix EMS mental health? There’s a crap ton we can do for that. But it can, should, and must start with properly stigmatizing and shunning anyone in EMS who thinks this is how we should treat each other. Because now these students and new hires think this is acceptable. IT. IS. NOT. ACCEPTABLE.